#Industry News
The transversus Abdominis muscle
The treatment of common low back pain is a regular spinal rehabilitation performed by physiotherapists.
In this rehabilitation approach, practitioners aim, within a specific number of sessions (up to 15 without prior patient consent [1]), to enable patients to become self-reliant in the use of the correct movements and postures for the post-rehabilitation phase. One of the keys to this learning process is the TrA. In this paper, we describe its anatomy, biological functions in relation to the associated clinical indications and the means of controlling its activity.
ANATOMY OF THE TrA
The TrA is an abdominal wall muscle presenting horizontal muscle fibres, hence its name. In general terms, it extends from the spinal column at the back towards the linea alba at the front.
The upper part inserts into the lower six ribs, as shown from the front. Depending on the individual, its insertion into the spinal column can be on the transverse processes of 4 or 5 lumbar vertebrae.
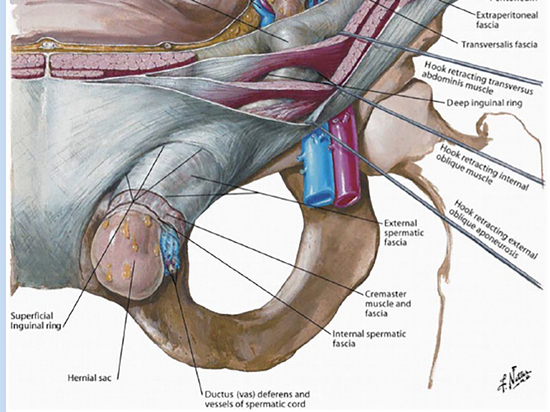
The lower part inserts into the internal aspect of the anterior 2/3 of the iliac crest and into 1/3 of the inguinal ligament. The insertions of the TrA make it an important muscle in spinal support but one that is not readily accessible.
Where it terminates, the TrA forms a wide aponeurosis that is fixed to the abdominal linea alba, which descends to the pubis. Its conjoined tendon with the internal oblique forms the inguinal falx.
It is the deepest abdominal wall muscle [2].
Its most superficial insertions are located at the conjoined tendon (inguinal falx) and at the inguinal ligament. The TrA is found in its most superficial position, on the lower third of the linea alba and, in particular, below the arcuate line of the ilium, since it passes in front of the rectus abdominis muscle and behind the internal and external obliques [2] [3].
BIOLOGICAL FUNCTIONS AND INDICATIONS
When it contracts, the transverse abdominis muscle acts by compressing the viscera onto the spine. This is especially the case during exhalation: its insertions onto the ribs draws them towards the median plane, reducing the thoracic volume [3].
This action means the TrA plays a key role in major biological functions: defecation, vomiting, childbirth, the respiration process and even reflex spinal support (in co-contraction with the multifidus) [2] [4].
◊ Postpartum abdominal rehabilitation
Pregnancy is a major biological event affecting several physiological processes. This is especially the case with the TrA, which becomes distended and therefore risks becoming inactive [13]. Several journals have reported a change in the behaviour of the abdominal wall muscles, and especially the pelvic floor muscles, after pregnancy. In particular, it has been shown that the interaction between the pelvic floor and the TrA changes during pregnancy, and during the postpartum period in first-time mothers [5]. In this context, exercises aimed at reconditioning the deep muscles of the abdominal wall in women after childbirth are important, as they help women towards their target objective of returning to “normal” condition (including among other things, getting back their pre-pregnancy appearance) [5] [8].
Several types of exercises are recommended, including Abdominal Hypopressive Gymnastics, which work these muscle groups, while avoiding pelvic floor hyperpressure [13].
◊ Rehabilitation of obstructive, restrictive or mixed respiratory diseases
Due to its anatomical positioning, acting antagonistic to the diaphragm, the transverse adbominis plays a role in respiratory function in humans [6]. During an obstructive respiratory disease, such as COPD, it has been shown that the activity of the expiratory muscles, including the TrA, are proportional to the severity level of the pathology; as the activity of the expiratory muscles reduces, the pathology becomes more advanced [9]. In addition, having subjects work this muscle improves their respiratory capacity, while working on their spinal stability.
For this purpose, a study involving 22 subjects showed that the forced vital capacity and forced expiratory volume over 1 second, improved significantly in patients who practiced deep abdominal muscle strengthening exercises. [6]
◊ Spinal rehabilitation
One cannot talk about the TrA without mentioning its strong involvement in spinal stabilisation. Its anatomical positioning makes it an excellent natural belt, preventing spinal movement through reflex contraction before each movement involving the spine. This preventative contraction occurs within a period of around 1 second prior to effort in healthy patients. In patients suffering from low back pain, this period can be longer. Several studies have also shown a reflex loss and have emphasised the importance of practicing deep muscle strengthening exercises [4] [7].
To support this, it should be noted that the French National Authority for Health in its 2005 recommendations (most recently updated in 2018), emphasised the importance of masseur-physiotherapists in addressing subacute recurrent and chronic low back pain, in particular core and lumbo-pelvic muscle strengthening exercises [10].
ASSESSING Tr A CONTRACTION
Due to its positioning, it is very complicated to assess the activity of the TrA alone. Its deep position, as well as its most superficial insertions associated with the internal oblique, make accurate assessment difficult. In the context of rehabilitation, the objective of physiotherapists is to recruit as many TrA muscle fibres as possible.
Patient involvement is key, as is often the case. However, for TrA recruitment, it is hard to find an exercise that can enable patients to feel and acquire voluntary TrA contraction capacity. Several publications have shown that the most effective exercise in this respect is the draw-in [11] [12] [14]: patients contract the deep abdominal muscles, in particular the TrA, without recruiting the more superficial abdominal muscles (external oblique / rectus abdominis) or back muscles (erector spinae). Patients perform a forced exhalation by pulling the stomach inward, then inhale via the airways (visible by chest elevation). Physiotherapists assess the contraction at the moment of exhalation by placing their hand on the median plane of the anterior superior iliac crest [12].
Several publications have revealed the difficulty of confirming the correct performance of the exercise. In fact, patients often perform the exercise incorrectly and do not feel the contraction. This makes the practitioner’s explanation essential. In addition, there are few means of confirmation available to physiotherapists and these primarily involve palpation and observation of the correct positioning of patients before and during the exercise. However, an American study demonstrated the value of visual biofeedback while learning this exercise. Practitioners are equipped with an ultrasound generator, which enables them to visualise the contraction of the TrA in real time. [12]
It should nevertheless be noted that this method can only be used when patients are perfectly static, in a position in which the ultrasound probe can be used to access the anterior abdominal wall, which physiotherapists must keep it in a specific position while patients perform the respiration exercise, and that interpretation of the image displayed requires a good understanding of this imaging technique (moreover specific training is required), which decreases the scope of application of this method.
This article has been written and reviewed by Blueback together with Servane Cosqueric, Physiotherapist in France.
BIBLIOGRAPHY
[1] Guide pratique NGAP masso-kinesitherapie CSPR (page 16) - 5 février 2016
[2] Livre « Evaluation clinique de la fonction musculaire » – Lacôte/Chevalier/Miranda/Bleton – 4ème Edition 2010 Maloine
[3] http://imedecin.com/Muscles-de-l-abdomen/description-anatomique-du-muscle-transverse-de-l-ab-
domen.html
[4] Hodges et al. 1996 “Inefficient muscular stabilization of the lumbar spine associated with low back pain” – Spine
[5] Pereira et al. 2013 “Are Transversus Abdominis/oblique Internal and Pelvic Floor Muscles Coactivated
During Pregnancy and Postpartum ?” – Neurology and Urodynamics
[6] Stuge et al 2004 “The efficacy of a treatment Program focusing on specific stabilizing exercises for pelvic girdle pail after pregnancy” – Spine
[7] Kim et al. 2013 “The Effects of Deep Abdominal Muscle Strengthening Exercises on Respiratory Function
and Lumbar Stability” – Journal of Physical Therapy Science
[8] Selkow et al 2017 “Transversus Abdominis activation and timing improves following core stability training: a randomized trial” - International Journal of Sports Physical Therapy
[9] Stuge et al. 2004 “The efficacy of a treatment Program focusing on specific stabilizing exercises for
pelvic girdle pail after pregnancy” – Spine
[10] Ramirez-Sarmiento et al. 2002 “Expiratory muscle endurance in chronic obstructive pulmonary disease” – Thorax
[11] Recommendations de la Haute Autorité de la Santé dans la prise en charge masso-kinésithérapique
de la lombalgie commune - mai 2005
[12] Richardson et al. 1999 “Therapeutic exercise for spinal segmental stabilisation in low back pain.
Scientific basis and clinical approach” - 1st edn. UK: Churchill Livingstone
[13] Henry et al. 2005 “The use of Real-Time Ultrasound Feedback in teaching abdominal Hollowing Exercises to healthy subjects” - Journal of Orthopedic&Sports Physical Therapy
[14] Ithamar et al. 2018 “Abdominal and pelvic floor electromyographic analysis during abdominal
hypopressive gymnastics” – Journal of Bodywork and movement therapies