#Product Trends
ROBOTIC-ASSISTED SURGERY: FIVE MISCONCEPTIONS AND THE FACTS BEHIND THEM
You’ve recently received news you’ll be needing surgery. The best option, according to the surgeon, is through robotic-assisted surgery or RAS.
What, exactly, is RAS? Are they robotic surgeons with tentacles for arms that shapeshift into lethal-looking scalpels and needles? Or microbe-sized robots that infect human cells to transform them per programming from a secret government institution?
The reality is much less fantastical than the descriptions above. Here are five misconceptions about surgical robots and the facts behind them.
Misconception: The Surgery is Performed by Robots
Fact: The surgery is performed by the surgeon
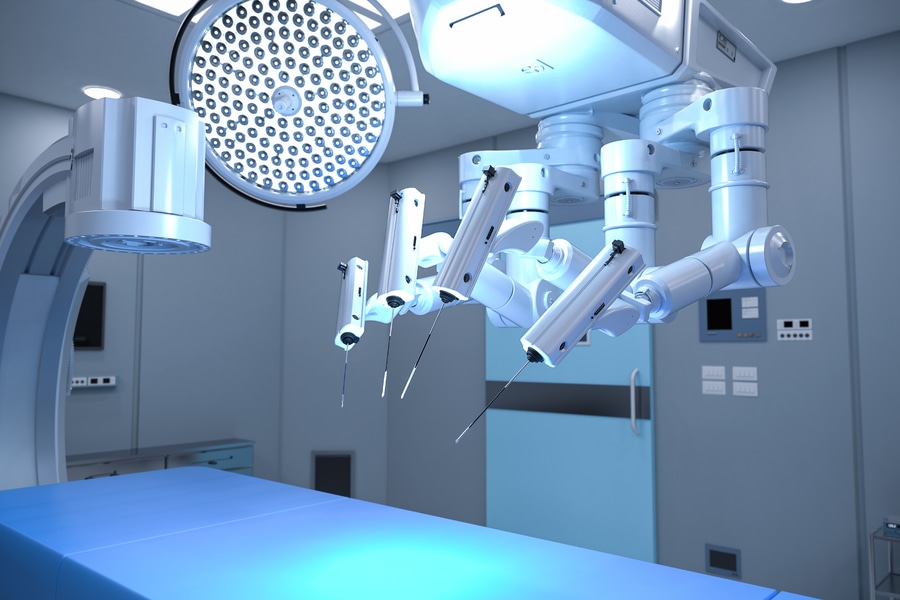
This is the most common misconception. Simply, RAS is a tool like a scalpel, forceps, EKG machine, or medical tablet. The surgeon controls the various precision-guided robotic arms that hold and manipulate miniaturized instruments using hand and foot controls. The process can be summarized as:
The surgeon makes one or more small incisions into the patient’s body.
They place thin tubes called ports into the incision. The robot is attached to these ports.
A camera system called an endoscope is placed through one of those ports. This allows the surgeon to have a highly precise, 3D view of the area.
Surgical instruments necessary for the operation are placed through the other ports.
The surgeon watches through the endoscope and controls the various arms to perform the operation. Normally, they are sitting a few feet from the patient. (Though surgeries can be done remotely.)
An assistant stands nearby and helps by changing the instruments as required.
Misconception: RAS is a New Technology
Fact: Robots have been used for surgical procedures since the 80s
The PUMA 560 is considered the first RAS. The robotic surgical arm was first used in 1985 during an open surgery. In 1997, a robot called Mona assisted Dr. Jaques Himpens of Belgium in a cholecystectomy (the removal of a gallbladder).
Robot-assisted surgery technology saw a leap forward in 2000. That was the year the FDA approved the da Vinci Surgical System, the most well-known RAS. Also that year:
Dr. Arnold Advincula performed one of the first robotic-assisted hysterectomy (removal of a uterus) in the US.
The Zeus RAS system was used by New York-based physicians to perform a cholecystectomy to a patient located in France.
Misconception: There is Very Little Difference Between RAS and Traditional Surgery
Fact: There are many advantages
The title says it all. Many are based on the fact that much smaller incisions can be made using RAS than traditional surgeries like laparoscopic or ﹘ especially ﹘ open. This results in:
Lower risk of infection
Reduced blood loss
Smaller scars
Hospital stay is shorter
Less pain for patients recovering from procedures
Telehealth is another advantage. The Zeus mentioned earlier showcases this, which simply cannot be done using traditional surgeries. And how is this good? Well, in 2014, researchers from both New York-based Mount Sinai Health System Icahn School of Medicine and the Umea University in Sweden did studies on the feasibility of RAS done remotely. There were two studies, one on conducting ultrasound exams while the other for echocardiogram. They showed, among other things, diagnostic processing time dropped from an average of 114 days to 27 while wait time for patients to see a specialist plummeted from 86 days to 12.
Clinicians are hopeful that such results can further increase patient satisfaction especially in hard-to-reach places like farms.
Another advantage: surgeons suffer less fatigue using RAS. Operations can last for hours. Surgeons have to stand the entire time in most of them. Worse, they have to bend, twist, and turn to get their numerous surgical tools into the right positions.
RAS largely eliminates these body movements, which is very beneficial. As Dr. Gerard M. Doherty, surgeon-in-chief at Brigham and Women’s Hospital in Boston, points out:
“There is this ergonomic advantage. We move the arms of the robot while sitting comfortably. I have one surgeon who told me it will extend his career by a decade.”
Myth: RAS is Virtually Risk-Free
Fact: A surgeon’s skill primarily determines the risk, not RAS
A paper published in the Agency for Healthcare Research and Quality points to the surgeon’s skill as the primary reason for complications when using RAS. It showed, though, that those with greater familiarity with the technology like RAS performed better than those without but with equal skill. In the study, Adverse Events in Robotic Surgery: A Retrospective Study of 14 Years of FDA Data, which was published in 2016, the researchers concluded:
“Despite widespread adoption of robotic systems for minimally invasive surgery in the U.S., a non-negligible number of technical difficulties and complications are still being experienced during procedures. Adoption of advanced techniques in design and operation of robotic surgical systems and enhanced mechanisms for adverse event reporting may reduce these preventable incidents in the future.”
At the same time, risks from technology can’t be fully ruled out. There is always going to be some risk when using medical devices. Consider:
A legacy anesthesia machine could be displaying the wrong information to the anesthesiologist’s medical computer.
An infusion pump could leak because it was refurbished through a third-party medical device manufacturer instead of its OEM.
For RAS systems like da Vinci, computer errors resulting in electric arcs to instruments freezing up or moving out of control have been documented. Same with extremely rare complications like electric burns, large blood loss, and punctured organs and other vital tissues.
Experts say in many cases, 30 percent were the result of device failure, followed by:
Incorrect device operation setup (25 percent)
User error (20 percent)
Other (11 percent)
Inadequate training (7 percent)
Maintenance issues (7 percent)
Misconception: Surgical Robots are Just a Fad
Fact: The market looks to grow
The da Vinci Surgical System by Intuitive Surgical Inc. is currently the dominant OEM of surgical robots. It will face more competition from other manufactures as demand continues, as well as the introduction of new technologies like augmented intelligence for virtual assistants for surgeons.
And that competition looks to grow big. The market for surgical robots worldwide was estimated to be $6.4 billion in 2021. Research firms like Markets and Markets project demand will reach $14.4 billion by 2026 and more than $20 billion by 2030.
Closing Thoughts
Which of the above facts did you find interesting about robotic-assisted surgery? Would you take it if it was offered to you? Or prefer traditional surgical techniques?
Contact an expert at Cybernet if you’re interested in learning more about the role of robotic-assisted surgery for your medical group.