#Product Trends
Full arch restorations with Z1 implants
Régis Nègre discusses an implant case in which the patient specifically wanted a non-removable solution
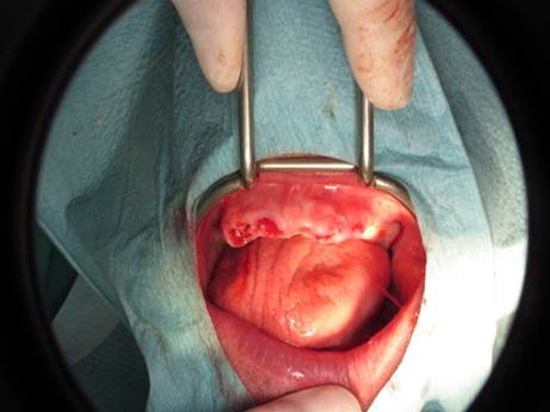
A 51-year-old female patient presented to the practice with a heavily restored and highly compromised dentition (fig 1-3). She specifically requested a non-removable solution – something which other practitioners in the area had not been able to provide for her – on account of her profession as a butcher and her fondness for sausages: she had not been able to enjoy eating these with her current dentition and she believed a removable option would not be suitable.
After assessment, it was found that the patient exhibited a noticeable loss of vertical dimension, which meant that implant therapy was the most suitable approach for treatment in order to recreate the posterior occlusion. It was also found that the remaining teeth in her upper arch were in such poor condition, with deep apical infection, that complete extraction was the only option (fig 4). The extracted teeth would be replaced with six implants and a screw-retained bridge.
On the lower arch, in which some of the patient’s remaining teeth were suitable for preparation and restoration, it was decided that a combination ofimplant retained bridges and unitary crowns, along with traditional crowns, would be sufficient to restore function.
This was duly explained to the patient who provided informed consent and treatment commenced.
Initially, two impressions were taken in order to simulate on the articulator the vertical dimension and final fit of the future prosthetic restoration. A method of guided surgery was planned, whereby the implant placement would be guided by the resulting prosthesis. This approach allows for an accurate final fit that conforms with the patient’s natural occlusion.
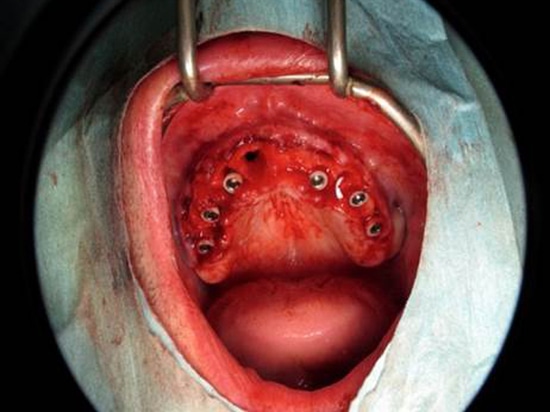
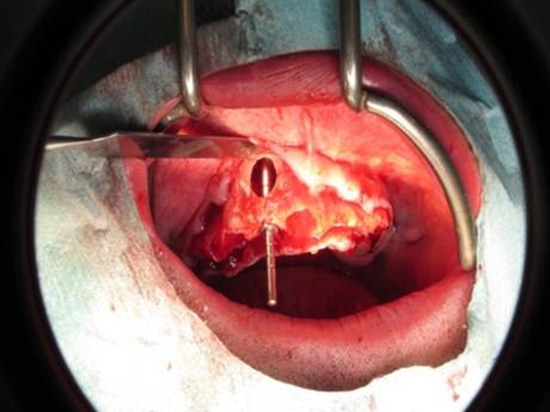
The teeth of the upper jaw were extracted and, using the aforementioned surgical guide, six TBR Z1 tissue-level implants were placed (figs 5-7). Due to a previous cyst in the UR7 position – and the resulting cavity in the maxilla – the apex of the implant did not have the preferred stability (fig 8). However, the rest of the treatment site did have sufficient bone volume and density to ensure sufficient primary stability. Bone augmentation was duly undertaken in the cavity and the results have been more than acceptable.
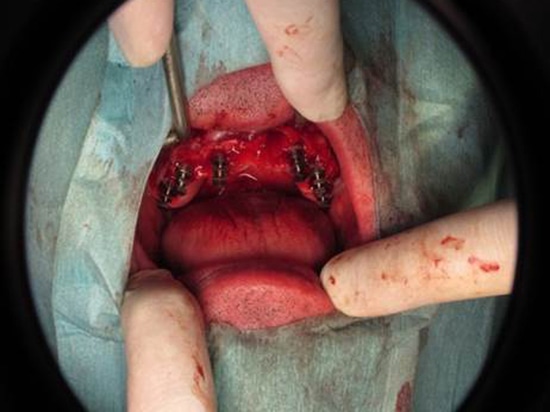
Before suturing, a simple impression was taken using TBR SwissClip impression posts (fig 9). This is a much faster approach than screw-retained pick-ups and both expedites the impression process and affords greater patient comfort.
Once the impressions had been taken, sutures were placed around the zirconia collar of the Z1 implant, readying them for placement of the screw-retained temporary prosthesis in two days. In total, the surgery took approximately an hour to complete.
Two days later, in the patient’s next appointment, the patient exhibited good initial healing – with normal and acceptable inflammation of the gingiva (fig 10) – and the Zirkonzahn resin temporary bridge was fitted. At this early stage, the immediate screwretained temporary can be used to gently adapt the implants’ position on the bridge, since complete osseointegration would not have taken place.
Four Z1 implants were placed in the lower jaw and a temporary bridge was placed onto the patient’s natural teeth to enable function during the healing period (figs 11 and 12).
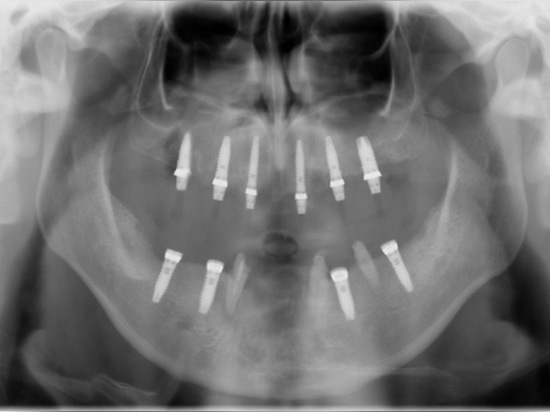
After four months, the patient was recalled and a control X-ray was taken to check the position of all implants (fig 13). All 10 implants were exhibiting good osseointegration and, thanks to the Z1’s unique zirconia collar, excellent soft tissue healing.
Working above the gingiva with tissue-level implants like the Z1 enables simpler procedures and soft tissue preservation, stabilisation and management.
Eight months after initial surgery the final lower jaw prostheses were fitted. The decision to cement both traditional and implant-retained restorations was made to avoid the use of screw-channels and improve overall aesthetics. Again, thanks to the Z1’s zirconia element, cement retained restorations are predictable and efficient. The tissue level zirconia collar creates an antimicrobial barrier that reduces the risk of peri-implantitis and enables a more accurate limit for the crown.
The lower jaw restoration was comprised of five different elements – a combination of bridges and unitary crowns and all created in full zirconia. This was done to avoid joining implant retained and tooth retained restorations (fig 14).
The temporary on the upper jaw was left in place for several more months in order for the patient to set their ideal occlusion. Due to the friction imposed on the resin of the upper bridge by the harder lower restoration, a map of the occlusal forces was created for when the patient came in for the final fit to create the best possible upper bridge (fig 15).
The final full zirconia bridge was fitted after three more months – a total of 11 months after initial surgery (figs 16 and 17).
The patient is incredibly happy with the result and has had full function restored.
Régis Nègre is a dental surgeon practising in Rodez, France. He has been successfully placing Z1 implants for over 15 years.