#Product Trends
Best implant for the site
Régis Nègre shows how and why the zirconia collar tissue level implant is the best
A 38-year-old male patient presented having lost his central incisor due to untreated periodontitis. He was a smoker, but was aware that without quitting and without undergoing full periodontal treatment, the implant treatment he needed could be compromised. As such, the patient quit smoking before treatment commenced.
There are three key factors highlighted in the literature that need to be respected when looking to place a dental implant at the same time as performing guided bone regeneration (GBR):
1. The height and thickness of the buccal plate should be at least 3mm (Araujo et al, 2006; Tomasi, 2010)
2. The minimum distance between the implant and the neighbouring natural teeth should be 2mm (ITI Team, 2007)
3. A tissue level implant should be placed 1mm beneath the cementoenamel junction of the neighbouring natural tooth. For bone level implants, they should be placed 3-4mm under this junction (Palmer et al, 2003).
We know that a one-step implant surgery affords improved stability of the peri-implant soft tissue and, consequently, higher stability of the bone as well. Professor Rompen suggested in 2017 that a biocompatible transgingival component should be fitted immediately after implant placement. This component should not be removed again in order to avoid tearing the junctional epithelium cells that have attached to the component. This concept is called ‘one abutment – one time’ (Santos et al, 2018).
In the author’s opinion, why shouldn’t we say that the best implant is therefore the zirconia collar tissue level implant, which, once it has been placed, doesn’t require any additional manipulation of the gingiva? The following case presentation will show that only one surgery with a tissue-level implant combining titanium and zirconia, even for a complex case like this, is the answer to modern implant dentistry.
Case presentation
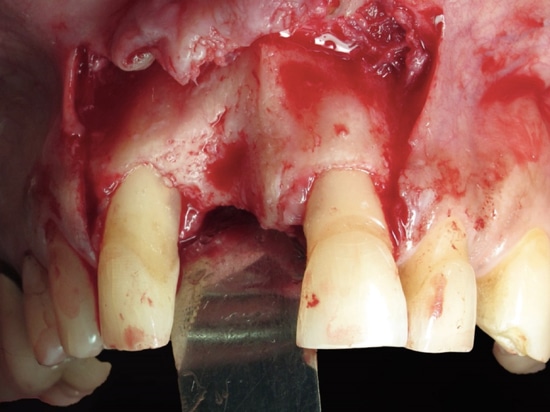
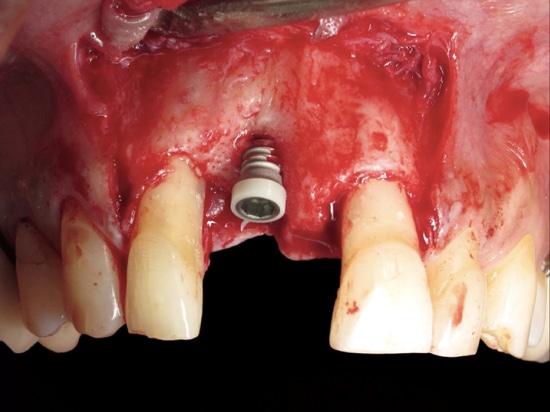
Figure 1 shows the initial situation as the patient presented.
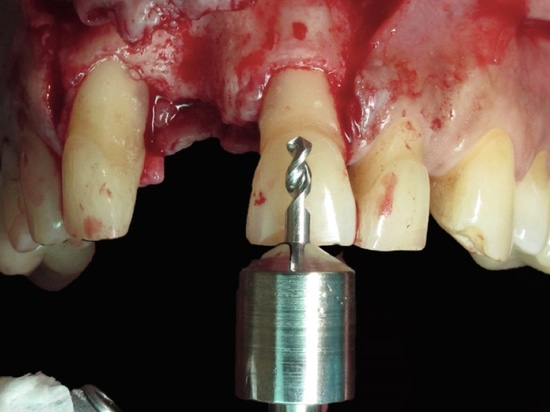
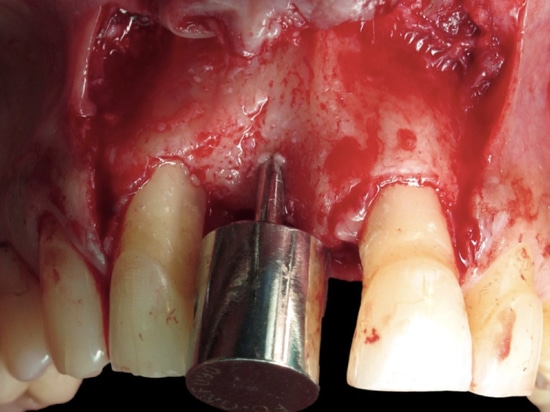
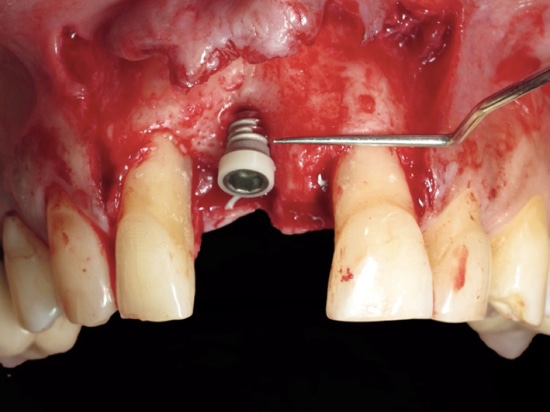
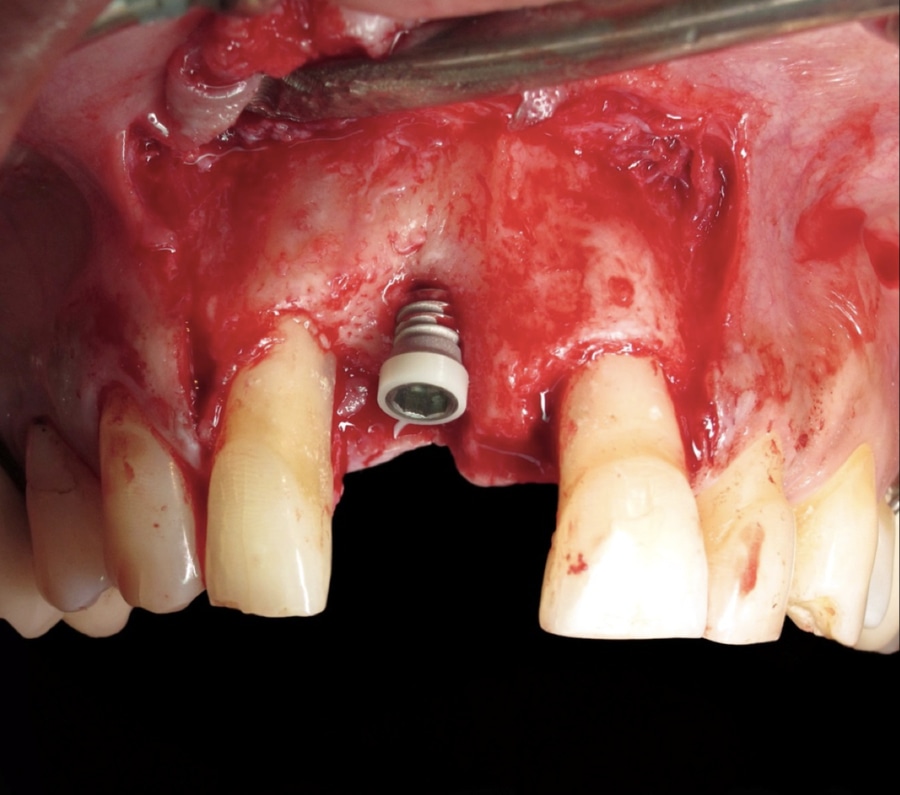
An incision was made slightly more towards the adjacent tooth (Figure 2) in order to encourage the most effective vascularisation for the future GBR. A drilling guide and initial drill from TBR Implants was used (Figure 3), which is designed to allow the clinician to achieve the ideal mesialdistal position of the implant. The purpose of this initial drill is that the shoulder has the same diameter as the tooth to be replaced, further ensuring ideal implant position (Figure 4). It also allows us to respect the safety distance from the
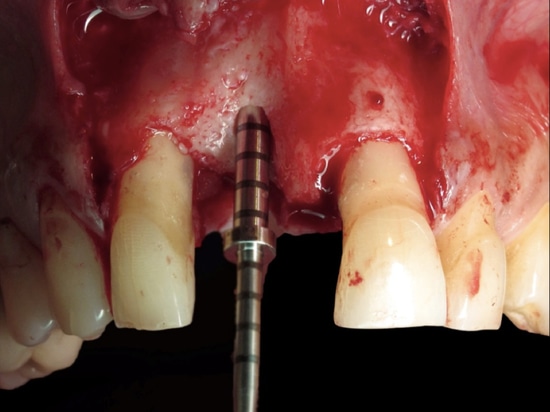
neighbouring teeth, as stated earlier. In addition, the drilling depth was controlled so as to ensure the zirconia collar was located 1mm below the crown of the adjacent tooth, as recommended in the literature (Figures 5 and 6).
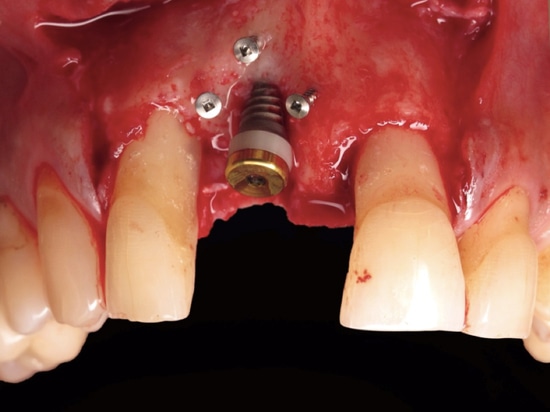
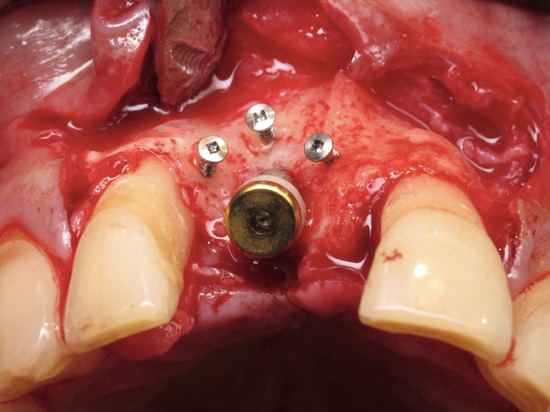
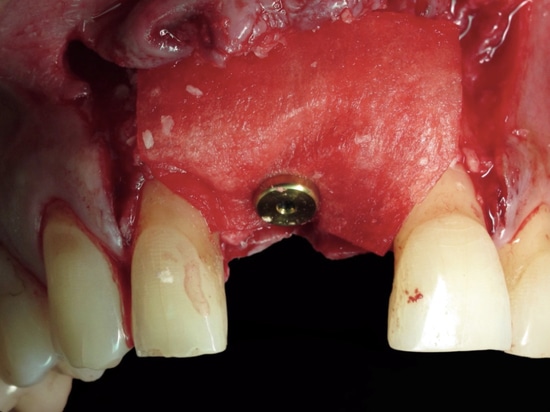
In order to obtain perfect symmetry with the left central incisor, the titanium part of the Z1 implant placed needed to be covered with bone on the buccal side (Figure 7). Moreover, the GBR needed to recreate the 3mm thickness of buccal bone that is necessary for the survival and aesthetic result of the implant. For this, three osteosynthesis screws were used to support the reconstructed bone (Figures 8 and 9).
An allogenic graft was performed using a mixture of cortical cancellous granules and I-PRF, according to the protocol designed by Dr Joseph Choukroun (Figure 10) (Miron et al, 2017). A collagen resorbable membrane was placed and stabilised with the implant cover screw (Figure 11). This compensated for the slight bone resorption that we would expect during the healing stage – it is generally accepted that the vertical bone loss is around 1mm when we perform GBR (Covani et al, 2007).
An A-PRF membrane was placed over the top of this (Figure 12) – once again in accordance with Dr Choukroun’s protocols – to improve healing of the peri-implant tissue and protect the GBR (Ghanaati et al, 2014). This technique enables us to avoid performing a connective tissue graft, which would require a second surgical site, more advanced surgical skills and increased chair time.
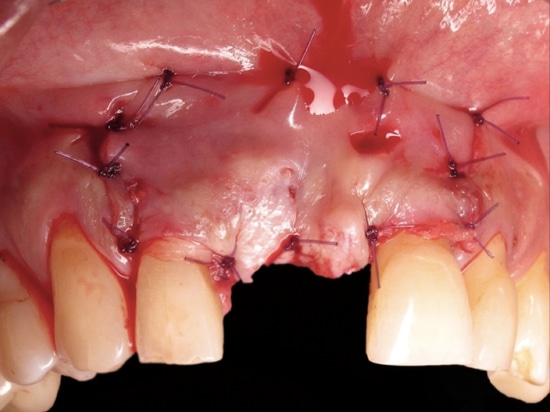
To increase elasticity of the flap, reduce tension once the flap was closed and prevent the need for a half-thickness flap in the first place, the ‘soft tissue brushing’ technique was used. Ultimately, this is a softer technique for the patient, leading to increased comfort and less bleeding for improved healing, plus, it is less invasive. The flap was stabilised using apical mattress stitches (Figure 13).
Four months post-surgery, the soft tissues had healed well around the implant (Figures 14 and 15). An electric surgical blade was used to remove a small amount of the soft tissue and allow for a more accurate impression procedure. This is another benefit of working with a transgingival zirconia collar – unlike ceramic, zirconia is an ideal electrical insulator.
The final abutment was then fitted (Figure 16), followed by provisional cementation of a full zirconia crown that was stratified on the buccal side (Figure 17) – all prosthetic work was completed by Dr Iri Ayako. At a review two months later, the greyish tinge that could be seen at four months above the crown, had disappeared completely.
Dr Régis Nègre is a dental surgeon practising in Rodez, France and is part of TBR's expert training team.
References:
Araujo MG, Wennström JL, Lindhe J (2006) Modeling
of the buccal and lingual bone walls of fresh
extraction sites following implant installation.
Clin Oral Implants Res 17(6): 606-614
Tomasi C, Sanz M, Cecchinato D, Pjetursson B, Ferrus
J, Lang NP, Lindhe J (2010) Bone dimensional
variations at implants placed in fresh extraction
sockets: a multilevel multivariate analysis.
Clin Oral Implants Res 21(1): 30-36
International Team for Oral Implantology (ITI)
Consensus Conference. Vitznau, Switzerland, 1997.
Proceedings. Clin Oral Implants Res 11
(Suppl 1):1-158
Palmer RM, Palmer PJ, Newton JT (2003) Dealing with
esthetic demands in the anterior maxilla.
Periodontol 2000 33:105-18
Santos JS, Santos TS, Martins-Filho PRS, Krockow NV,
Weigl P, Pablo H (2018) One Abutment at One Time
Concept for Platform-Switched Morse Implants:
Systematic Review and Meta-Analysis.
Braz Dent J 29(1): 7-13
Miron RJ, Fujioka-Kobayashi M, Hernandez M,
Kandalam U, Zhang Y, Ghanaati S, Choukroun
J (2017) Injectable platelet rich fibrin (i-PRF):
opportunities in regenerative dentistry?
Clin Oral Investig 21(8): 2619-2627
Covani U, Cornelini R, Barone A (2007) Vertical crestal
bone changes around implants placed into fresh
extraction sockets. J Periodontol 78(5): 810-815
Ghanaati S, Booms P, Orlowska A, Kubesch A, Lorenz
J, Rutkowski J, Landes C, Sadar R, Kirkpatrick C,
Choukroun J (2014) Advanced platelet-rich fibrin:
a new concept for cell-based tissue engineering by
means of inflammatory cells. J Oral Implantol
40(6): 679-89