#Product Trends
Interrupted Aortic Arch (IAA)
What Is Interrupted Aortic Arch?
Interrupted aortic arch (IAA) is a rare but life-threatening congenital heart defect characterized by a complete discontinuity of the aorta at the level of the aortic arch. This interruption prevents normal blood flow from the left ventricle to the lower part of the body.
Under normal conditions, the heart consists of four chambers: two atria and two ventricles. The left ventricle pumps oxygenated blood into the aorta, which forms the aortic arch, supplying the head, brain, and upper extremities through its branches before continuing downward as the descending aorta to perfuse the lower body and legs.
In patients with interrupted aortic arch:
• The aorta is divided into two separate segments
• The proximal aorta supplies blood to the head and upper limbs
• Blood flow to the lower body depends on the pulmonary artery via a patent ductus arteriosus (PDA) or other fetal circulatory pathways
Without prompt intervention, this abnormal circulation is incompatible with survival after ductal closure.
How Does Interrupted Aortic Arch Develop?
IAA results from abnormal development of the embryonic aortic arches during early fetal life. Specifically, failure of certain primitive vascular arches to grow and fuse properly leads to interruption of the aortic arch.
In some cases, genetic factors are involved. The condition is most commonly associated with DiGeorge syndrome, caused by a microdeletion on chromosome 22 (22q11.2 deletion). However, many patients have no identifiable genetic abnormality.
Pathological Classification
Interrupted aortic arch is classified into three types based on the anatomical location of the interruption. Although clinical manifestations are similar, the anatomical differences are critical for diagnosis and surgical planning.
Type A
• Interruption site: Distal to the origin of the left subclavian artery
• Incidence: Approximately 55% (most common type)
Type B
• Interruption site: Between the left common carotid artery and the left subclavian artery
• Incidence: Approximately 40%
• Clinical relevance: Most frequently associated with DiGeorge syndrome
Type C
• Interruption site: Between the innominate artery and the left common carotid artery
• Incidence: Approximately 5% (rarest type)
Clinical Presentation
Most infants with IAA become symptomatic shortly after birth, particularly as the ductus arteriosus begins to close. Common signs include:
• Severe respiratory distress
• Cyanosis
• Poor feeding and lethargy
• Weak or absent lower-extremity pulses
• Metabolic acidosis and shock
IAA is considered a neonatal cardiac emergency.
Diagnosis and Evaluation
Early diagnosis is critical. When IAA is suspected prenatally or after birth, immediate evaluation is required:
1.Echocardiography – the primary diagnostic tool to assess aortic continuity and associated defects
2.Cardiac CT or MRI – provides detailed anatomical visualization and aids in classification
3.Cardiac catheterization – used selectively for hemodynamic assessment and surgical planning
Treatment Strategies
Management of interrupted aortic arch requires rapid stabilization followed by definitive surgical repair.
1.Emergency management
• Continuous infusion of prostaglandin E1 to maintain ductal patency
• Careful transport to a specialized pediatric cardiac center
• Supplemental oxygen is often avoided to prevent premature ductal closure
2.Surgical repair
• Definitive surgery is performed urgently or semi-urgently after diagnosis
• The procedure involves reconstruction of the aortic arch and correction of associated cardiac anomalies
In experienced pediatric cardiac centers, surgical success rates exceed 95%, and long-term outcomes are generally favorable.
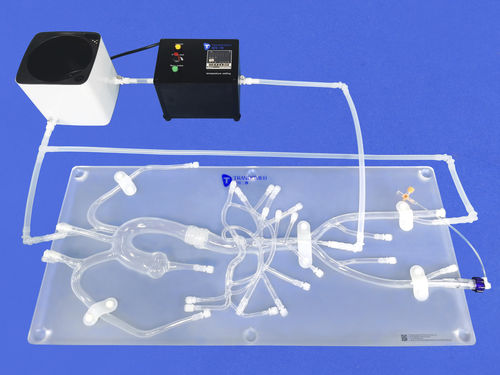
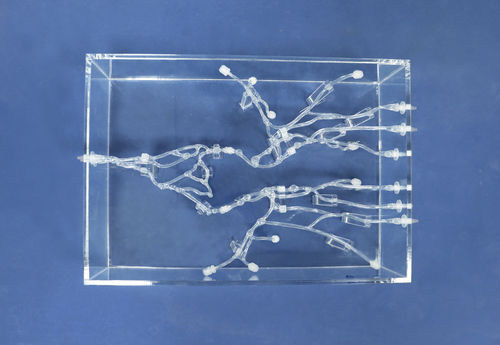
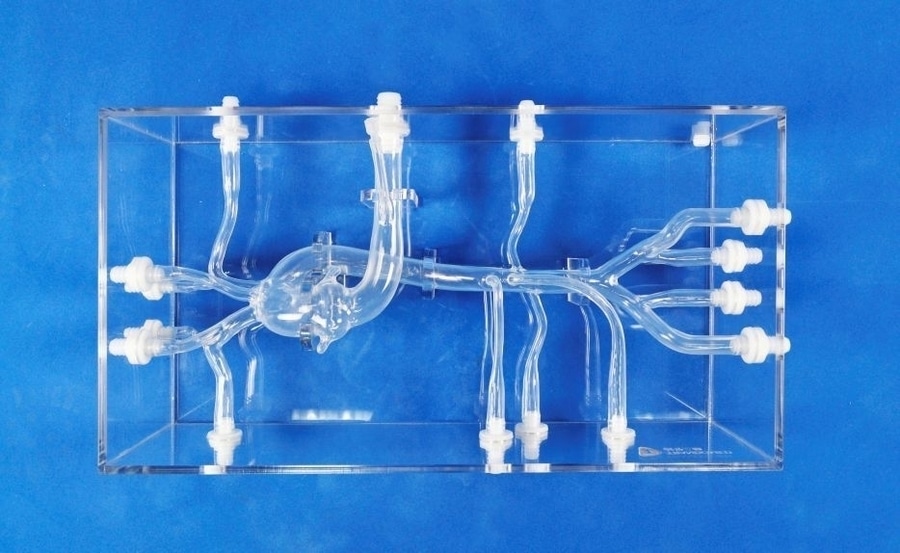
Our aortic arch model is designed to help users better understand the anatomical structure of the aortic arch. It can be customized to simulate different arch configurations, allowing realistic visualization and procedural simulation across a variety of anatomical scenarios.