#Product Trends
Pulmonary Atresia (PA)
Also known as Pulmonary Valve Atresia
Pulmonary valve atresia is a congenital heart disease characterized by fusion of the pulmonary valve leaflets into an imperforate membranous structure, resulting in obstruction of blood flow between the right ventricle and the pulmonary artery. The condition is classified into two main types: pulmonary atresia with intact ventricular septum and pulmonary atresia with ventricular septal defect. The former is often associated with interatrial communication and patent ductus arteriosus (PDA), while the latter is commonly accompanied by tetralogy of Fallot–like anomalies.
The etiology includes both functional factors (such as pulmonary hypertension) and structural factors (such as rheumatic disease and congenital malformations). Diagnosis mainly relies on echocardiography, ventricular pressure measurement, and angiography, with different diagnostic strategies applied according to the specific subtype.
Classification of Pulmonary Atresia
Pulmonary atresia is classified into four main types, based on pulmonary artery development, pulmonary blood supply, and the presence or absence of a ventricular septal defect (VSD).
Type I: Pulmonary Atresia with Intact Ventricular Septum (PA/IVS)
• Anatomy: Complete pulmonary valve atresia with a normally developed main and branch pulmonary arteries; no VSD
• Pulmonary blood supply: Dependent on PDA or minor collateral vessels
• Clinical features: Severe cyanosis and respiratory distress shortly after birth due to ductal closure
• Management: Emergency maintenance of ductal patency (e.g., prostaglandin E1), followed by staged interventional or surgical treatment.
Type II: Pulmonary Atresia with Ventricular Septal Defect (PA/VSD)
• Anatomy: Pulmonary valve atresia combined with VSD; pulmonary arteries are often hypoplastic
• Pulmonary blood supply: Mainly supplied by major aortopulmonary collateral arteries (MAPCAs)
• Associated anomalies: Frequently associated with tetralogy of Fallot–like features
• Treatment challenges: Requires complex, staged surgical reconstruction of pulmonary arteries and collateral integration
Type III: Absence of the Main Pulmonary Artery
• Anatomy: Complete absence of the main pulmonary artery; left and right pulmonary arteries arise directly from the aorta or collateral vessels
• Pulmonary circulation: Entirely dependent on systemic circulation
• Complications: High risk of pulmonary hypertension and progressive pulmonary vascular disease
• Prognosis: Surgical correction is highly complex; some patients may only be candidates for palliative treatment
Type IV: Unilateral Pulmonary Artery Atresia or Absence
• Anatomy: Atresia or absence of one pulmonary artery (commonly the right), with relatively preserved development of the contralateral pulmonary artery
• Pulmonary blood supply: The intact lung supports the majority of pulmonary circulation
• Treatment strategy: Focuses on optimizing blood flow to the functional pulmonary artery; interventional closure of abnormal collaterals may be considered
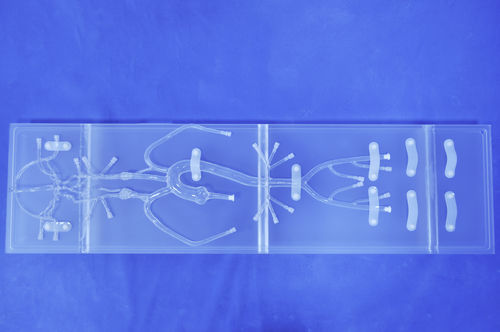
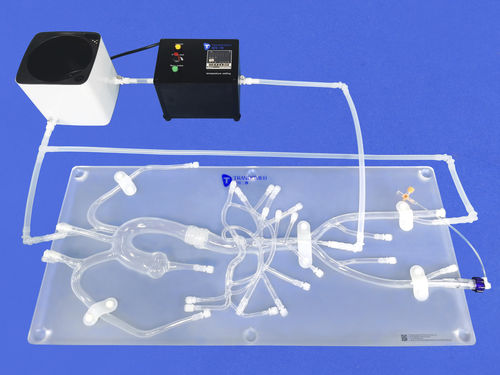
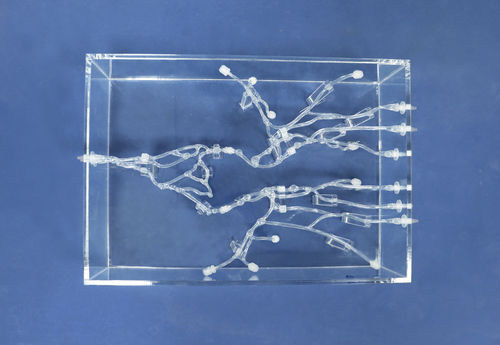
In this heart model with valves, we can incorporate a pulmonary valve with pulmonary atresia. Our model is designed to help you better understand the anatomical features and pathophysiology of pulmonary atresia, and to support the simulation of procedural and surgical treatment approaches for this condition.