#Product Trends
One-Minute Guide to the Full Process of Coronary Angiography
One-Minute Guide to the Full Process of Coronary Angiography
Coronary angiography is an essential skill for medical students, residents, cardiologists, interventional physicians, radiologists, technicians, nursing staff and cath lab teams.
Given its high operational difficulty, radiation exposure and potential complications, simulation training has become indispensable for relevant medical practitioners. This article summarizes the complete procedural steps of coronary angiography, including anatomical basics, standard workflows and image interpretation for your reference.
1. Preoperative Preparation
1.1 Patient Assessment & Informed Consent
Indications: Clarify examination purposes, such as diagnosing chest pain, evaluating myocardial ischemia, and preoperative assessment for PCI.
Contraindication Screening: Screen for contrast media allergy, renal insufficiency (caution if eGFR<30), uncontrolled infection, and severe coagulation disorders.
Preoperative Examinations: ECG, echocardiogram, blood routine, coagulation function, renal function (creatinine, urea nitrogen), and infectious disease screening.
Medication Adjustment: Discontinue metformin to prevent contrast-induced nephropathy; adjust anticoagulant medications if needed (e.g., stop warfarin for 3 days).
1.2 Patient Preparation
Fasting and water restriction: 4–6 hours of fasting and 2 hours of water deprivation to avoid vomiting and aspiration during surgery.
Skin preparation: Clean the puncture site (radial artery or femoral artery area).
Venous access: Establish peripheral intravenous access on the contralateral upper limb.
1.3 Equipment & Medication Preparation
Cath lab devices: DSA system, ECG monitor, defibrillator and oxygen supply system.
Catheter selection: Judkins catheters (JL/JR series) are widely used; Amplatz or multi-purpose catheters for complex anatomical structures.
Contrast agent: Low-osmolar non-ionic contrast media (Iohexol, Iodixanol) to reduce nephrotoxicity.
Intraoperative heparinization: Intravenous injection of 2,000–5,000U unfractionated heparin.
2. Detailed Surgical Procedures
2.1 Puncture & Vascular Access Establishment
Radial artery (preferred): Abduct the forearm, locate arterial pulsation, and perform puncture via modified Seldinger technique.
Femoral artery: Puncture 2 cm below the inguinal ligament; ultrasound guidance for obese patients.
Sheath insertion: Place a 5F/6F arterial sheath, connected with pressurized normal saline for continuous flushing to prevent thrombosis.
2.2 Catheter Advancement & Coronary Ostium Positioning
Trans-radial approach: Catheters pass through the brachial artery, subclavian artery, aortic arch and ascending aorta.
Trans-femoral approach: Direct catheter advancement to the aortic root.
Left coronary artery cannulation: Use JL catheter, rotate clockwise to engage the left coronary ostium.
Right coronary artery cannulation: Use JR catheter, rotate counterclockwise to access the right coronary sinus.
2.3 Contrast Injection & Image Acquisition
Projection angles: Standard views including LAO, RAO, cranial and caudal angulations to fully visualize LAD, LCX and RCA.
Contrast injection dosage: 6–8 ml for left coronary artery, 4–6 ml for right coronary artery.
Real-time monitoring: Assess vascular stenosis, lesions, collateral circulation and TIMI blood flow grade.
2.4 Emergency Management for Complications
Catheter impaction: Immediately withdraw the catheter if pressure waveform damping occurs.
Coronary spasm: Intracoronary injection of nitroglycerin (100–200μg).
Allergy rescue: Prepare epinephrine, dexamethasone and other emergency drugs.
3. Postoperative Management
3.1 Catheter Removal & Hemostasis
Radial artery: Apply dedicated compression devices with gradual decompression.
Femoral artery: Manual compression for 15–20 minutes followed by compression bandaging.
3.2 Postoperative Observation
Continuous vital signs and ECG monitoring for 2–4 hours.
Assess distal blood circulation and peripheral artery pulsation regularly.
3.3 Complication Prevention
Hydration therapy to reduce contrast-induced nephropathy.
Standard dual antiplatelet therapy to lower thrombotic risk.
4. Key Points for Image Interpretation
Coronary segmentation: 15-segment classification based on AHA standards.
Stenosis evaluation: Visual estimation and QCA quantitative measurement; stenosis ≥50% is defined as clinically significant.
Plaque identification: Distinguish calcification, ulceration and thrombosis to guide clinical treatment.
5. Common Mistakes & Learning Recommendations
Novices are prone to operational errors such as rough catheter manipulation, incomplete angiographic views and neglected hemodynamic changes, which may increase procedural risks.
High-frequency simulation training is strongly recommended for beginners.
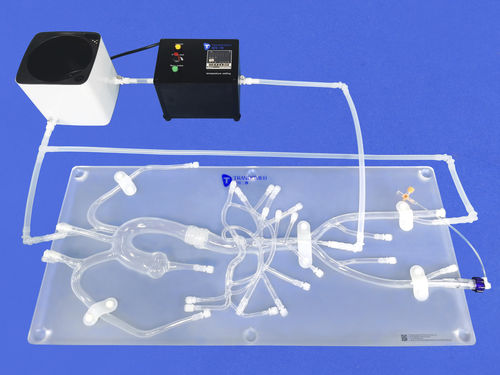
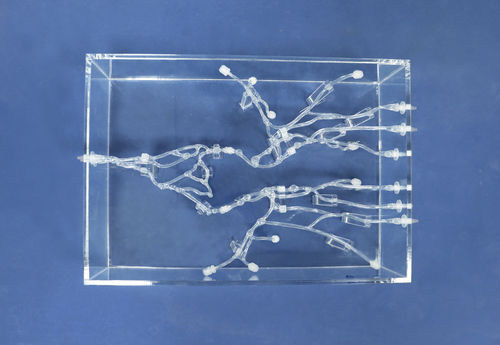
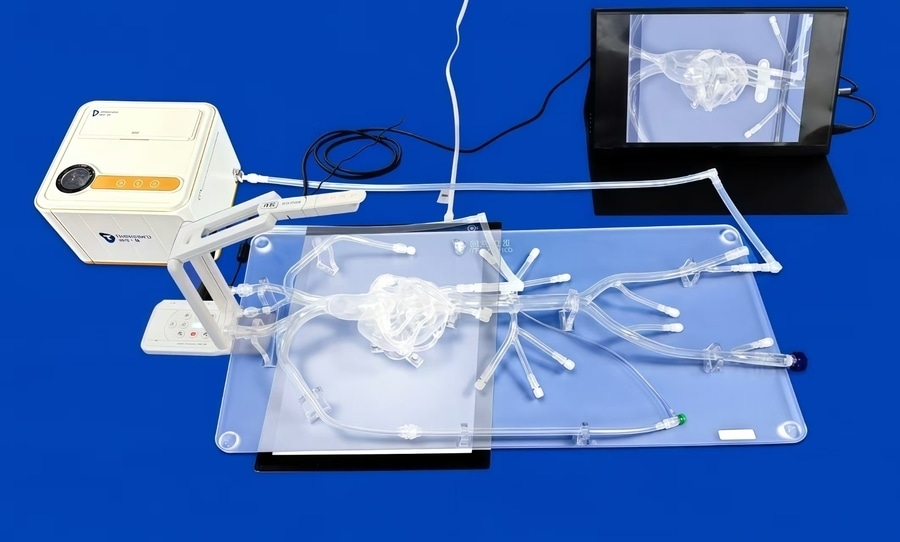
High-fidelity interventional training models are widely adopted for coronary angiography and interventional operation practice.
6.Trandomed
Our simulation models integrate radial artery puncture, coronary vascular access and complete circulation systems to simulate human blood circulation. The transparent vascular design enables intuitive and visual simulation of the full coronary angiography procedure.